Enterprise Healthcare
The Last 100 ft of Medication Delivery
A systems-level investigation into infusion workflows that examined how verification, device interaction, and physical space intersect during bedside medication delivery.
Enterprise Healthcare
A systems-level investigation into infusion workflows that examined how verification, device interaction, and physical space intersect during bedside medication delivery.
The Challenge
This project began within Baxter’s R&D innovation program to explore workflow breakdowns at the point closest to the patient. Our focus: how digital systems, devices, and physical space intersect during infusion setup.
The goal was not feature refinement, but systems-level insight.

“Innovation distinguishes between a leader and a follower.”
Steve Jobs,
Discovery
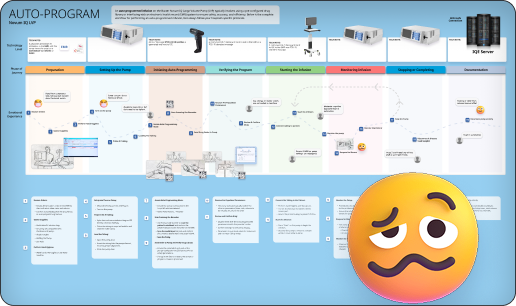
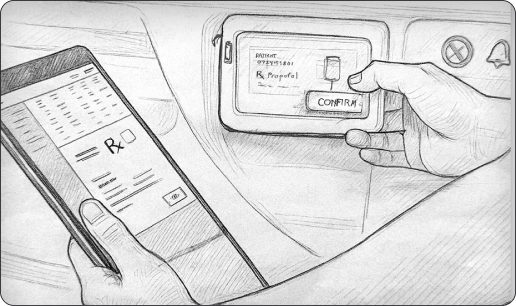
We documented the full auto-programmed infusion process across EMR, drug library validation, barcode scanning, pump programming, monitoring, and documentation.
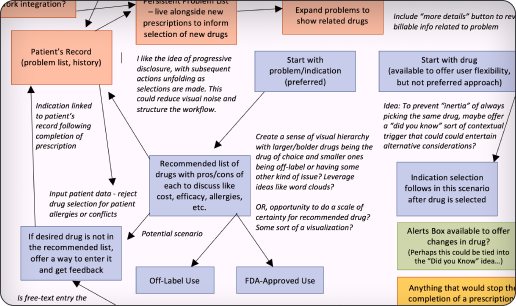
Mind mapping the infusion nurses’ complete process
The 19-step sequence was validated with clinicians. While technically sound, it revealed repeated verification and hidden complexity.
The system was safe — but not efficient.
An experience map created to identify pain points
Clinician Validation
The process map showed what happened — not where it happened.

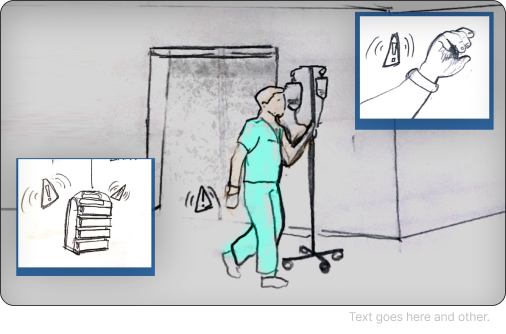
Infusion bag hanging in a medsurg unit of hospital.
Nurses moved repeatedly between workstation, patient, pump, and supply areas. The physical layout introduced friction invisible in the digital model.
This realization triggered a pivot
Deeper Discovery
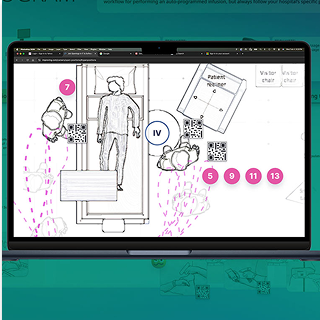
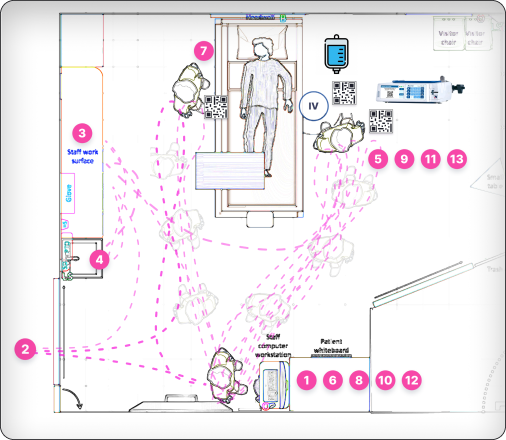
I translated the workflow into architectural room layouts and mapped clinician movement during infusion setup.
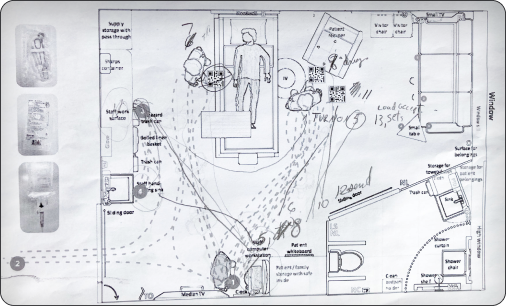
Ambulatory map in a standard “Med/Surge” hospital room
Across configurations, movement patterns repeated: back-and-forth walking, supply retrieval loops, and distributed verification steps.
The problem wasn’t just interaction design — it was spatial workflow design.
Text goes here and other.
Key Insights
Nearly every major step confirms:
Administration is secondary to validation.
Improvement required rethinking where verification happens — not removing safeguards.
Verifying the Workflow
Text goes here and other.
Administration is secondary to validation.
Improvement required rethinking where verification happens — not removing safeguards.
Ideation
After the initial review by the engineering team, clinicians, and directors. I was honored to be selected as the featured speaker at Baxter’s Innovation Day to present “The Last 100 ft of Medicine” and formally frame the problem space.

Images of the workshop break-out sessions.
The day began with a clear and comprehensive framing of the problem statement, streamed live to a broad cross-functional audience. Following the presentation, participants broke into smaller groups of 10–20 to explore the challenge through guided discussion and collaborative exercises.
The session reframed the final stage of medication delivery as a critical design opportunity, aligning teams around patient safety, workflow transparency, and systems-level thinking.
Feasibility
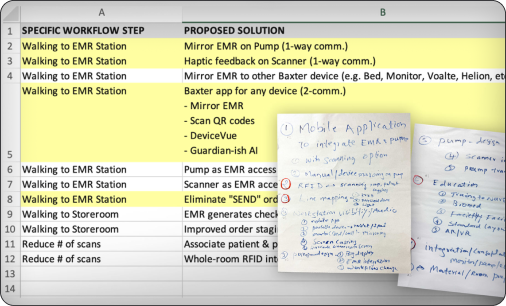
Innovation workshops explored how verification could be embedded closer to the bedside:
Concepts were filtered for feasibility and aligned with engineering constraints.
Text goes here and other.
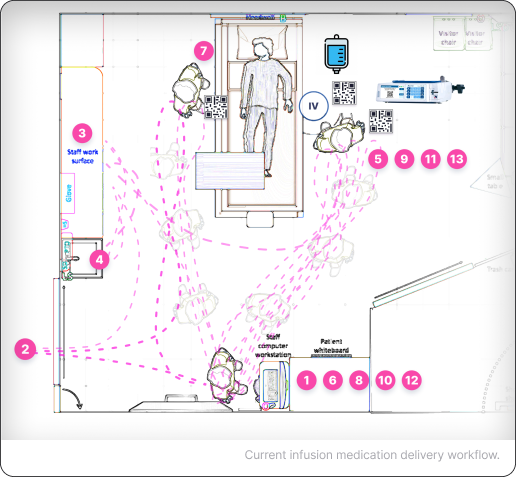
Current infusion medication delivery workflow.
Concept modeling of a Centralized Hub interaction approach reduced that to roughly 14 steps — over 50% fewer movements.
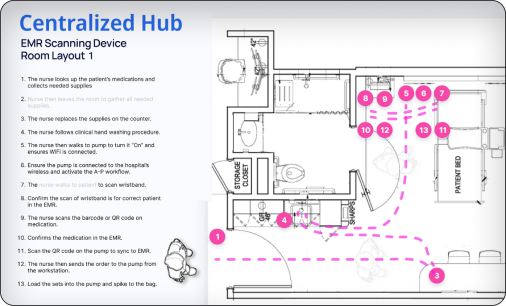
Revised Centralized Interaction Hub infusion medication delivery workflow.
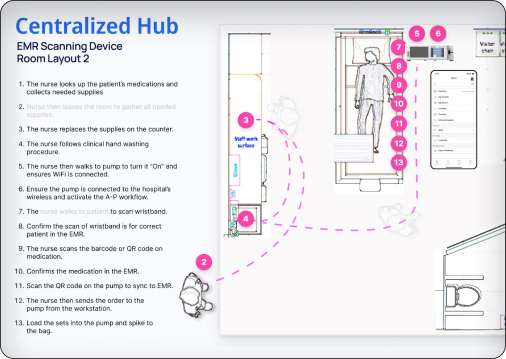
Revised Centralized Interaction Hub infusion medication delivery workflow.
Opportunity
Opportunities were mapped against difficulty and reward:
This reframed the work from ideation to roadmap thinking.
Text goes here and other.
Concept modeling of a centralized interaction approach reduced that to roughly 14 steps — over 50% fewer movements.

Text goes here and other.
Text goes here and other.
A validated end-to-end infusion workflow model
The conversation shifted from feature tweaks to systems-level redesign.

Text goes here and other.
Conclusion
This project explored the hidden inefficiencies in bedside infusion workflows. Through clinician interviews, direct observation, and spatial mapping, the study revealed that verification-heavy processes and fragmented physical interactions dramatically increased cognitive load and unnecessary movement—informing a reimagined, centralized interaction model.